Setting up and running explicit Mentalizing Groups 101: Simple guidance and Clinical considerations
Over the past decade, Mentalization Based Treatment (MBT) has risen to prominence as an evidence-based treatment for a variety of difficulties (Vogt & Norman, 2018). This paper offer offers simple guidance on setting up and running explicit Mentalizing Groups. It summarizes key aspects of the model. It suggests some minor changes to language used to describe the model to prospective group members which have grown out of clinical practice and also adds some suggestions about breaks and introducing new members derived from clinical experience in groups. It is aimed at novices to such groups. It is not suggested as an alternative to formal MBT training or group psychotherapy training, nor does it provide an in-depth introduction to mentalizing theory, which will be signposted throughout.
Mentalizing and Groups
Groups were an integral part of the original Mentalization Based Treatment (MBT) model as designed and researched (Bateman & Fonagy, 2009). Guidance for groups has been variously described: Karterud (2015) described a clinical model Mentalization-Based Group Therapy (MBT-G), giving us a glimpse of a whole MBT-G session and explaining its place in the family of group therapies; also introduced is a Quality Assurance tool, that can be used to ascertain whether groups are on task as Mentalizing Groups; Bateman & Fonagy (2016) provided detailed theoretical underpinnings of MBT and gave clarity to the clinical group model, concisely identifying therapist techniques; Inderhaug & Karterud (2007) tackled issues of therapist authority in the group; and Fonagy, Campbell & Bateman (2017) explained the importance of epistemic trust within group therapy and provided guidance for its establishment and maintenance. Qualitative research on service user experience in group psychotherapy (Hummelen, Wilberg & Karterud, 2007) identified some issues in traditional group therapy (for some patients) which MBT sought to address. Service user experiences in MBT groups were explored by Dyson & Brown (2016) and Lonargain, Hodge & Line (2016).
The aim of Mentalizing Groups
First thing Tyler yells is, “The first rule about fight club is you don’t talk about fight club. “The second rule about fight club,” Tyler yells, “is you don’t talk about fight club.” (Palahniuk, 1997: 50)
If we were to draw a comparison with Mentalizing groups, paradoxically, we probably would not be talking about ‘rules,’ because rules imply ‘black and white’ certainties which jar with an idea of maintaining a thoughtful but ‘not-knowing’ position. If we were to agree that aims are coherent to mentalizing thinking, however, the rules might translate as:
The first aim of mentalizing group is to promote mentalizing; the second aim of mentalizing group is to promote mentalizing.
Mentalizing
According to pioneers of Mentalization Based Therapy (MBT) Bateman and Fonagy:
Mentalizing describes a particular facet of human imagination: an individual’s awareness of mental states in himself or herself and in other people, particularly in explaining their actions. It involves perceiving and interpreting the feelings, thoughts, beliefs, and wishes that explain what people do. This entails an awareness of someone else’s circumstances, his or her prior patterns of behaviour, and the experiences to which the individual has been exposed.(Bateman & Fonagy, 2019: 3)
Put very simply, Mentalizing is an imaginative activity that helps us understand the mental states of ourselves and others; and to understand people’s actions and behaviour.
Other definitions explain it as thinking about feeling and feeling thoughts; seeing ourselves from the outside and others from the inside; and holding minds in mind (Bateman & Fonagy, 2019)
Mental states are simply the feelings, thoughts, beliefs, values, needs and desires that people have. We might also understand that those mental states arise in response to certain driving forces or factors including biology and genetics; life experiences; past relationships (including early attachments with caregivers); trauma; and also, a wide range of social factors, including our culture, group history and spirituality. It is important to understand that mental states are opaque, therefore any attempt to understand them is on the basis of our inferences, which is why mentalizing is descried as an imaginary process.
Bateman ad Fonagy (2016) explain that the capacity to mentalize:
‘is not an entirely stable, consistent, or one-dimensional thing. We are not all able to mentalize to the same extent; many of us have strengths or weaknesses in particular aspects of mentalizing, and most of us are more likely to struggle to mentalize in moments of stress or anxiety.’
(Bateman & Fonagy, 2016: 5)
One way of thinking about the quality of mentalizing is to look at it dimensionally: Lieberman (2007) explains that mentalizing can be characterised as falling along 4 poles or opposites. Holding the task of promoting consistent and effective mentalizing in mind, breaking the poles down into a 3+1 model (fig. 1) , provides a roadmap for using them in therapy.
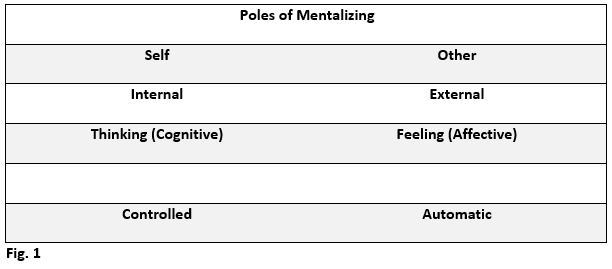
Using this model, we aim to achieve balanced mentalizing across poles of self / other, internal / external and thoughts (cognitive) / feelings (affective) whilst maintaining as consistent a focus, as possible, on controlled mentalizing on a pole of automatic / controlled. Given the link between thoughts, feelings and distress; another way is to consider their impact on mentalizing; under-arousal of thinking and feelings (hypo-mentalizing) makes mentalizing difficult (can’t think, can’t find words, numb, cut-off, zoned out or dissociated); conversely, over-arousal (hyper-mentalizing) is likely to lead to breakdowns in mentalizing (overwhelmed by thoughts and feelings, meltdowns, explosions, ruminations). I sometimes use a cooking metaphor here: too little or too much seasoning can render a dish unpalatable; the right balance of seasoning makes it tasty.
Under optimal circumstances, mentalizing develops naturally in the context of secure attachment relationships with primary caregivers (Fonagy & Luyten, 2009). By mirroring the infant’s mental states, often in a marked or exaggerated way and through ostensive cues (clear), caregivers are able to foster ‘epistemic trust’ (trust in the context of relationship which opens the mind to acquiring knowledge and skills) (Fonagy & Allison, 2014), the infant co-constructs with (an) other, then develops, an understanding of their minds and the minds of others. Where this process has not occurred or has been interrupted, e.g. through trauma, the therapeutic task is to restore the capacity to develop mentalizing by encouraging and practising it in healthy trustworthy therapeutic relationships, and to build emotional and relational stamina which can then be generalized to real world living.
Pre-Mentalizing Modes
As a developmentally acquired skill, mentalizing succeeds pre-mentalizing modes of regulating emotions and understanding ourselves and others. These pre-mentalizing modes persist in people whose mentalizing has not developed well. It is also evident in most people when mentalizing fails or breaks down. Bateman & Fonagy (2016) describe 3 discreet categories of pre-mentalizing or non-mentalizing modes, and their developmental origins: psychic equivalence, teleological mode and pretend mode. When introducing mentalizing to prospective group members, a personal use of simplified language has been adopted to introduce the ways in which people see the world and regulate emotions when they are struggling:
Equivalence Mode (psychic equivalence in mentalizing literature) is when the perspectives of our minds and others are confused and believed to be equal. Such thinking tends to be fixed, inflexible and concrete (‘all knowing’). It can involve a dogmatic worldview (‘black and white thinking’). It tends to be over-generalized e.g. you must be thinking or feeling what I am thinking you are thinking or feeling. It can include ‘time collapse’ when events or feelings from one time are confused with the present – Bateman and Fonagy write of 90/10 events (Lewis, Kelly & Allen, 2004) when a large proportion of responses rightly belong to past situations and relationships, and only a small proportion seem appropriate to current ones. Such responses are sometimes termed transferential and may relate to early attachment patterns; Sometimes, in this mode, the present becomes a certain view of the future. Equivalence mode can seem very emotionally charged to the person in it and can evoke strong feelings in others – feelings of anger, frustration or a desire to argue another view.
Action Model (teleological mode in mentalizing literature) is when actions are used to understand and regulate emotion. In this pre-mentalizing mode, ‘actions speak louder than words.’ These actions can be by self or other. Such actions can include the use of alcohol, drugs, self-harm, under or over-eating, sex, gambling, and other potentially risky or harmful behaviours. It can involve dissociative states or some psychosomatic symptoms. It can also include seemingly healthy help seeking e.g. heavy reliance on healthcare professionals to provide diagnosis and medication; or healthy activities or coping strategies e.g. exercise, mediation, mindfulness or distraction techniques. It may involve seeking actions by others including their responses or presence to regulate emotions. Whilst action by self or others can regulate emotion in this mode, Inaction by self- or others, or delayed action can be associated with increased distress. The desire to ‘do something’ and a sense of urgency is often associated with action mode by both the person in it and others, including healthcare professionals (a feeling ‘I need to do something!’). This response has been termed ‘the righting reflex’ (Miller & Rollnick, 2002: 20). In groups, a common response is group members moving to advice giving, which should be acknowledged and explored.
Pretend Mode involves a disconnect between thoughts and feelings. It can sometimes be the hardest non-mentalizing mode to spot as it often appears ‘thoughtful.’ In pretend mode, often speech or narrative lacks emotion. This is often evident in assessment when someone sounds as if they are reading their life events from a script but without feeling. Sometimes affect seems inappropriate e.g. when sometimes describes trauma and smiles or laughs. People prone to pretend mode often report previous unhelpful experience of therapy (‘I know why I feel like x, it’s because of y. So why do I still feel like this?’) or they may talk ‘recovery’ but still struggle in therapy or their outside lives (‘talking the talk, not walking the walk’). Less kind descriptions of pretend mode include ‘psychobabble’ or ‘bullshit mode.’ It is important to note, however, that pretend mode is not a conscious way of relating, more a psychological defence mechanism, and people in pretend mode are generally trying hard to engage with the therapeutic process. People using pretend mode will often end up in long detailed descriptions of things, but a common response in others is boredom or struggling to concentrate or remember what was said.
Mentalization Based Treatment
Mentalizing was identified by Fonagy, Luyten & Bateman (2015) as a treatment target for people who meet the criteria for Borderline (BPD) or Emotionally Unstable Personality Disorder (EUPD) (BPD and EUPD refer to the same diagnosis using different diagnostic systems), as they seem to consistently demonstrate poor or inconsistent mentalizing and suffer high levels of relational conflict and distress.
Mentalization Based Treatment (MBT) (Bateman & Fonagy, 2006) was developed to address this unmet need. Initially, a day-hospital based intervention, the model was modified and researched as an outpatient treatment comprising assessment, psychoeducation and a treatment phase combining individual and group therapies. Since then, the model has been applied to and researched for a variety of diagnoses and presentations (Vogt & Norman, 2018). It is also routinely delivered in range of treatment forms including the original model MBT, psychoeducational groups, and other mentalizing informed therapies (individual, group, couples and family interventions). Mentalization Based Treatment Groups (MBT-G) is generally used to describe the group component of MBT programmes and group-only treatment as a Mentalization Based Treatment programme. The explicit Mentalizing Groups described in this paper are coherent with a mentalizing model.
Groups as a ‘Training Ground for Mentalizing’
There is arguably no definitive way to run a mentalizing group. Many therapy groups will promote mentalizing either implicitly or vicariously (Karterud, 2015), however, in Mentalizing Groups, the aim is made explicit. Some groups advertised as MBT-G, in clinical practice, may, in reality, more likely encourage mentalizing more implicitly than explicitly and operate with less structure than described here. Foulkes, a pioneer of group analysis once described group analysis as ‘ego training in action’ (Foulkes & Anthony, 1975) on account of improved ego function and sense of self which occur in group members over therapy. More recently, Karterud (2015), a pioneer of mentalizing in groups described how groups are a natural ‘training ground for mentalizing’ on account of the in vivo interpersonal events (and breakdowns in mentalizing) that occur in group therapy. Groups also provide peer-learning and feedback which may be more epistemically ‘trustworthy’ for people whose trust in parental or authority figures has been eroded through poor past experience (Karterud, 2015 and Fonagy, Campbell & Bateman, 2017).
A starting point for Mentalizing Groups
To ensure that prospective group members know what to expect from therapy and are signed up to that shared task, it is essential that potential group members are prepared for the group via an assessment of mentalizing and via an introduction to the key concepts and ideas associated with mentalizing. An Introduction to MBT (MBT-I) is described in Bateman & Fonagy (2016). In clinical practice, possibly, a pared down version of this covering Mentalizing, Non-Mentalizing, Emotions, Attachment, Mentalizing difficulties, and why groups might be especially helpful as training ground for mentalizing, may suffice.
To optimise therapeutic focus, potential members meet with group therapists prior to joining a mentalizing group and agree therapy aims. For Mentalizing Groups, these should be formulated in terms of relationships and improving consistent mentalizing.
Preparation should also include both mentalizing and practical expectations of group membership. Mentalizing expectations support the notion that ‘the first aim of mentalizing group is to promote mentalizing.’
Karterud (2015) suggested that the following is conveyed to potential recruits. It may be something that therapists wish to incorporate into a therapy agreement:
• You have to be willing to talk about relevant experiences from your own life, that is, take the initiative to bring events that are connected to your problems with mentalizing;
• You will have to explore these events in a mentalizing manner;
• You have to make an effort to relate to others in the group in a mentalizing manner;
• You have to make an effort to find out what is happening in the group and between group members in a mentalizing manner;
• You have to make an effort to attach to the group and its members.
The following expectations might also be shared:
• All instances of action mode including self-harm or suicidal behavior or the use of alcohol, substances or other harmful behaviors should be discussed in group.
Bateman & Fonagy (2016) added a further proviso that:
• people should agree not to problem solve (as it may indicate action / teleological mode and is not a mentalizing activity).
Practical Member Expectations might include:
• Regular attendance and notification of absence;
• Group members are expected to maintain confidentiality (including social media and blogs /vlogs);
• Use of phones in session;
• Treat others with respect and compassion;
• No violence;
• Don’t attend group intoxicated;
• Share time with others – good mentalizing is not about ‘talk time’;
• Extra-group (out of group) contact restrictions or guidelines.
For online therapy groups the following also need to be addressed:
• Recording and Screenshots – members should not record any part of sessions, including screenshots and therapists should ensure that if sessions are to be recorded for supervision or research that explicit consent is obtained;
• Locality – is the space suitable and the group not likely to be overheard or disturbed?;
• Agreements about what do when children, pets or devices require attention;
• Dress code – would members attend an in-person group at a clinic in nightwear for example?;
• Screen names – If out of group contact between members is an aspiration, then first names only should be used for screen names;
• Pre-group tests to ensure people can access the platform via their devices and connections are advised.
Confidentiality
The basic guideline for confidentiality in groups is that ‘who you see and what is said’ should remain confidential. Active engagement in therapy is not just time in group, and ideally group members will try to mentalize their everyday lives, and also reflect on the events of group, outside of group. This may involve reflecting with others, like partners, families and friends. To allow for this vital reflection, we might modify the ‘who is seen and what is said’ to make sure any reference to group and members is anonymized and the descriptions of content avoided e.g. explaining to a partner or other that you were upset in or after a group because difficult content was discussed but not talking about specific group members or repeating their life-stories. It would might also be OK to reflect on particular actions including verbal and non-verbal behaviours that evoke strong responses in someone and how they react to them – again, anonymously.
What can be talked about in Mentalizing Groups?
Anything can be talked about in Mentalizing Groups, so long as an attempt is made to do so in a mentalizing way. Karterud (2015) proposes that priority is given to emotionally charged interpersonal events, and this is certainly a helpful over-arching principle (first aim of Mentalizing Group is to promote mentalizing!).
Mentalizing self-harm and suicide attempts
Like other evidence-based approaches for personality disorder e.g. Dialectical Behavioral Therapy (DBT) (Linehan, 2014) or Transference Focused Psychotherapy (TFP) (Yeomans, Clarkin & Kernberg, 2015), it is probably helpful to make acts of self-harm (especially life-threatening ones) subjects for a culture of curiosity or enquiry (Main, 1983). This is especially important in running groups in statutory settings like the NHS but is also good general clinical practice. Mentalizing both a person’s mental state but also the mental states of people around them including healthcare professionals is encouraged.
Mentalizing other harmful ways of coping
Using actions (in self or others) including the use of alcohol, substances and restricting / purging to regulate emotions (teleological mode) is a non-mentalizing activity and such behavior might form the basis of curious enquiry in Mentalizing Groups.
Talk-time in groups
A frequent anxiety in groups is that there will not be time to talk about ‘my stuff.’ This anxiety is real and often arises from people not having been listened to or heard in the past. This is something that could be mentalized. However, mentalizing is an imaginary activity which can be applied to our own life events or the life events of others. It is therefore possible to mentalize material in group even if it does not relate to us. This can even be done mentally, however, sharing our thoughts with others allows a richer understanding (co-mentalizing). Whilst not necessarily every week, it would be hoped that everyone in group will bring material over time which can be the focus for the discussion part of the group.
Therapeutic Interventions
In Mentalizing Groups, the first aim of therapists is to promote of mentalizing. This involves robustly, but compassionately, challenging non-mentalizing and re-starting the mentalizing process in group.
Therapists model a culture of ‘not knowing,’ curiosity and compassion. They regularly acknowledge that they are not ‘mind-readers’ or experts who automatically can discern the mental states of others, as mental states are opaque.
Therapists will offer structure to sessions allowing for time for affect focus; reflection of previous groups, time in between groups, and within sessions. They may also include time to mentalize risk or, in therapeutic community approaches solution focused goals and / or risk management.
Bateman and Fonagy (2016) suggested that groups should aim to follow the following trajectory: Summary of previous group; Problem ‘go around’ for all patients; Work towards synthesis, Exploration; Closure; Post-group discussion. In addition, to allowing time for mentalizing problems, this serves to establish a continuous and coherent narrative for the group (‘mentalizing the group’). Therapists use the post group meeting to agree and record a summary of the group for next time.
In addition, clinical experience has shown that beginning with an affect focused check-in (how do you feel right now?) encourages a curiosity in mental states from the outset and can give early indication of people’s mentalizing capacity for the beginning of the session. A similar check-out at the end, can provide interesting demonstrations of how mental states can change over an hour or so. It is also helpful for assessment and recording of risk.
The following session structure is therefore recommended:
• Check-in (Function: establishing affect focus – how are you feeling right now?);
• Recap on last week’s group (Function: narrative building – therapist led in early group stages, however over time, members can be encouraged to contribute);
• Issues to work on (Function: identifying breakdowns in mentalizing);
• Allocating time (Function: prioritization and encouraging pro-social behaviour);
• Discussion of material (Function: Mentalizing!);
• Summary of group including member reflections and validation of good mentalizing (Function: narrative building);
• Check out and risk ((Function: affect focus and risk management).
To hold the structure, an agenda or cheat-sheet, like those often used in Therapeutic Communities (TCs) (Pearce & Haigh, 2017) might be employed. The role of chairing the session is held by therapists, except in TC models, however, Bateman & Fonagy (2016) suggest that, over time, as the group matures, group members could be encouraged to contribute to the recaps and summaries – as well as bringing material and offering feedback in exploratory discussions.
Although, trying to promote balance across poles of cognitive/ affective focus, as many people seeking help find it difficult to identify and regulate feelings, it is likely, that therapists will often need to stimulate curiosity about affect. Whilst therapists often describe ‘following affect,’ it is important that people are steered away from ‘wallowing’ in feelings or getting stuck in them, as this form of mentalizing breakdown (hyper-mentalizing) is something we are trying to avoid in Mentalizing Groups.
Therapists should pay especial attention to over-arousal (hyper-mentalizing) or under-arousal (hypo-mentalizing) in group – if people are prone to frequent and / or lengthy dissociative states in group, this could become harmful in itself (iatrogenic) and consideration needs to be given to whether a group is helpful for that person at that time (they may need additional support e.g. grounding skills to help them obtain safe and effective use of the group).
Therapists aiming to promote mentalizing will probably frequently use ‘Stop, Rewind and Explore’ to move out of non-mentalizing by examining when mentalizing broke down in session. They may also use triangulation – introducing a third perspective into a dyadic exchange which is always directed at (an) other and not a general ‘what do others think?’ as this may inadvertently initiate advice giving or pretend mode in the group (Bateman & Fonagy, 2016).
In Mentalizing Groups, therapists will actively down-regulate high levels of conflict in group as this has been demonstrated to undermine group cohesion and has been linked to drop-outs (Hummelen, Wilberg & Karterud, 2007).
Sometimes, therapists will use ostensive cues or clear actions (like waving) to draw attention to them and stop the group in its non-mentalizing tracks.
This might involve ‘parking’ an issue or conflict that has become stuck and efforts to restart mentalizing have repeatedly failed (Bateman & Fonagy, 2016)
Mentalizing Group therapists avoid interpretations, especially whole-group interpretations, as such interventions are a non-mentalizing activity, moving out of the ‘not-knowing position into an expert one, knowing something the other doesn’t. Where therapists share their ideas or inferences, care must be taken to name them as such. Qualitative research (Malan et al, 1976) suggested that, for some people, bold whole-group interpretations, can undermine ‘epistemic trust’ by creating confusion and anxiety and making the group feel unsafe or unhelpful. In Mentalizing Groups, therapists only encourage mentalizing of ‘here and now’ relationships when people are mentalizing well – only linking current to past when there is a compelling reason to do so, and there is contemporary evidence to support it, of which the person is aware or appears close to awareness of.
Use of self – therapist transparency
Mentalizing Group therapists may talk through their own mentalizing in the group (often through exchanges with co-therapists) as modelling of a not-knowing or curious position (e.g. ‘I’m not sure what’s going on at the moment, I am finding it difficult to mentalize. What are you making of this?’).
Therapists are also encouraged to acknowledge their contributions misunderstandings or breakdowns in mentalizing (e.g. ‘how did you hear what I just said? or ‘did I inadvertently show shock or surprise?’).
How many people?
Although therapy groups can be any size, the small group of 8 seems to have become an accepted norm over the years for psychotherapy groups (Lorentzen, 2013)). Whilst Bateman and Fonagy (2016) suggest that MBT-G groups can be between 6-9 members, clinical experience suggests that a group of 6-7 achieves an optimal level of cohesion, intimacy and allows sufficient time for people to bring material on a not infrequent basis. Such numbers, however, may be difficult to justify, especially when 2 co-therapists run a group.
How long and for how long?
Traditional psychotherapy groups tend to be 90 minutes duration weekly. Given the focused nature of the mentalizing groups, clinical experience suggests 75 minutes is not over-taxing (remember we are aiming for controlled mentalizing for as long as possible as this seems more achievable in a slightly shorter group) – Bateman and Fonagy (2016) support this view.
Expert opinion used to be that short-term treatments (less than 9 months) should not be offered to people meeting a diagnosis of Borderline or Emotionally Unstable Personality Disorder (BPD / EUPD) because of a fear that attachment systems become activated, but the brevity of treatment doesn’t allow this to be worked through (NICE, 2009). However, therapies of less than 9 months have demonstrated effectiveness for people meeting the criteria for BPD / EUPD e.g. Cognitive Analytic Therapy (CAT) (Calvert & Kellet, 2014) and modified DBT skills groups (Valentine et al, 2015). Furthermore, in an RCT of short-term vs long-term group analytic psychotherapy, Lorentzen et al (2015) reported that whilst longer-term therapies achieved better outcomes for people meeting the criteria for PD, short-term closed group treatments still offer significant benefits, in terms of outcomes.
Running groups with co-therapists
In MBT programmes, it is common for 2 co-therapists to run the group. This can be really helpful as it provides multiple minds to mind the group, especially during difficult times. Whilst, idealized / demonized internal dynamics can be recreated in group (favoured / unfavoured therapists); having at least one therapist who is not ‘out of favour ‘can sometimes help people stay in group long enough to work through those dynamics. Working with co-therapists, however, can bring its own challenges and it is important to ensure that co-therapists get on, trust each other and complement each other’s style. Sometimes co-therapists divvy up tasks so that one will monitor quieter group members who are struggling e.g. watching for dissociation. It is possible to introduce novice therapists to therapy using co-therapists, and such clearly defined tasks provide good in-situ training opportunities. Co-therapists should aim to meet prior to and after the group to share mentalizing thinking and to ensure individual and group narratives are held in mind and a session summary is recorded.
Open versus closed groups
Closed groups which start and end with the same membership and everyone starting and finishing together can help the group develop high levels of groups cohesion and allow for high levels of trust to develop allowing for the exploration of potentially difficult and shameful material. Closed groups can be easier for novice therapists to set up and members are likely to negotiate stages of group development (Mackenzie, 1994) more or less together. However, closed groups can lead to long waits between groups for potential members to join a group, especially if recruitment of suitable group members is difficult. Working to a closed group start date can lead to poor group recruitment in terms of allowing high levels of ambivalence, to the Mentalizing approach or groups, to make up numbers. This can lead to early dropouts which can lead to the group becoming ineffective therapeutically or from a resource perspective.
Open groups offer the possibility of the most suitable members joining an established group when there is a space and when they are ready. Qualitative research (Dyson & Brown, 2016; Lonargain, Hodge & Line 2017) suggests that some people find the uncertainty of new members challenging at times. Over time, this can abate, and other people have recognized the benefits of thinking and feeling losses when senior members leave the group and the excitement and re-energizing effect that new members can bring a flagging group.
Qualitative research (Dyson & Brown, 2016; Lonargain, Hodge & Line , 2017) report that, regardless of whether a group is open or closed, some people report that the first six months of group are the most difficult and care should be taken to down-regulate conflict to minimize dropouts.
Therapy breaks
Therapy groups often have planned breaks. For people who struggle with problematic family dynamics, such breaks can occur when people need most support and thinking space. Offering groups on Mondays, when many public holidays fall, should be given careful consideration; as should commencing a group programme just before a planned therapy break. Using Co-therapists, breaks can be minimized however, it is arguable that trialing being without therapy, albeit for a short period, can have therapeutic value (rehearsing for life without therapy) and be something which can be mentalized in group. If running closed groups, consideration should be given to when a group will end. Is it a good idea to end a group just before a major holiday period? It may be a better idea to ensure that the group has a month or so after any major break before ending.
Introducing new members to an open group
In open groups, new members join, as old members leave. It is probably a good idea to allow a break between someone leaving and a new member joining so the group can mentalize an ending or loss.
In open groups, it can sometimes be helpful to introduce 2 members at the same time, so people don’t feel like the only new person – therapists are encouraged to be vigilant for the interrogation of newcomers.
If possible, introduce new group members at least one group after the first group back after a break as the first group back has the potential to be very busy and it is possible for new members to feel overlooked or overwhelmed.
All new members ending date should be held in mind from the outset and similar consideration around endings just before or immediately after public holidays or therapy breaks given to all members joining open groups.
Consideration should be given to issues of difference. Many people seeking help may have past experience of feeling like outsiders in their family and in groups. They may also have experienced discrimination and exclusion. The ‘Social GGRRAAACCEEESSS’ (Burnham, 2013) allow a framework to think this through. Having other members with shared characteristics can mitigate this, as can finding other areas in which people are similar. This should be addressed in group preparation. People must not be denied therapy because of their characteristics, however ensuring people are not alone in their difference, is encouraged, as otherwise groups can inadvertently function as iatrogenic re-enactments of discrimination and exclusion.
Individual Contact with group members
Where group is not combined or concurrent with individual therapy, consideration might be given to offering individual contact with the group therapist(s) if people are struggling to use the group. Where possible, this should be discussed in group before and after such meetings.
Reviews
Regular reviews can help maintain a therapeutic focus for members. They can occur in the group, as a therapeutic activity, or individually with the group therapist(s) where they can be a good place to think about issues which they have identified as important but which a person is struggling to bring to group. Every 3 months seems timely, with especial consideration given to the final review before leaving. Sometimes, therapists offer follow-up reviews to people 6-12 months after leaving group.
Supervision
Regular supervision of group work is essential. Where ‘expert’ supervision is not available, the supervision group should remind themselves of the aims of the group (the first aim of the group is to promote mentalizing!). Role plays and exercises can be helpful, as can viewing or listening to recordings of sessions, if this is possible. Using Quality Assurance tools can provide a framework for keeping therapy on task.
Quality Assurance
MBT and MG are not manualized, in the same way as some other treatments however, quality assurance can be maintained using QA tools such as those detailed in Karterud (2015). The MBT QA manual can be downloaded from the Anna Feud Centre website.
Online Groups
Current world events have focused the minds of psychological therapists on ways of delivering therapy remotely. Whilst no evidence on online MBT or Mentalizing Groups currently is published, Bateman and Fonagy (2019) propose that Mentalizing coherent therapies are likely to be helpful interventions. This is broadly in line with meta-analyses of psychotherapies which suggest that theoretically coherent and well-delivered treatments are likely to be effective (Wampold, 2015; Bateman & Fonagy, 2016). Lopez et al (2020) found that, for online DBT groups, whilst group cohesion was reportedly affected, satisfaction outcomes were broadly comparable with in person treatment. It is therefore conceivable that online groups will be helpful interventions, so long as they are coherent with a mentalizing model and conducted safely.
Family and Friends
Offering psychoeducation to family and friends on mentalizing and how treatment works has been shown be helpful in terms of engaging the whole system in the project of improving mentalizing and changing unhelpful dynamics which maintain a dysfunctional status quo. Such interventions are very popular with family and friends and can support people to engage with and stay in treatment. It is also possible that offering this in a multi-systemic format (person struggling plus partners, family or friends) could be beneficial. Teaching materials for a family and friends programme are detailed in Bateman & Fonagy (2016) and available from the Anna Freud Centre website: https://www.annafreud.org/training/mentalization-based-treatment-training/families-and-carers-training-and-support-programme-facts/ .
Conclusion
Mentalizing Groups coherent to the mentalizing model have the potential to be effective treatments (Wampold, 2015; Bateman & Fonagy, 2016; Vogt & Norman, 2018). Mentalizing, in itself is a simple concept, although for many people seeking help, it can be difficult to achieve and maintain consistently. With the guidance provided here, and elsewhere, competent therapists, even novices, could consider offering mentalizing groups, with the aim of promoting improved mentalizing within clinical settings and thereby add an evidence coherent treatment to their portfolio of available treatments.
References
Bateman, A. & Fonagy, P. (2009). Randomized controlled trial of outpatient Mentalization-Based Treatment versus Structured Clinical Management for borderline personality disorder. American Journal of Psychiatry, 166 (12), 1355-1364.
Bateman, A. & Fonagy, P. (eds) (2019). Handbook of Mentalizing in Clinical Practice (second edition). Washington, DC, American Psychiatric Association Publishing.
Burnham, J. (2013). Developments in Social GGRRAAACCEEESSS: visible-invisible, voiced-unvoiced. In I. Krause (Ed.), Cultural Reflexivity. London: Karnac.
Calvert, R. & Kellett, S. (2014). Cognitive analytic therapy: A review of the outcome evidence base for treatment. Psychology and Psychotherapy: Theory, Research and Practice, 87, pp 253-277.
Dyson, H. & Brown, D. (2016). “The experience of mentalization-based treatment: an interpretative phenomenological study”, Issues in Mental Health Nursing, Vol. 37 No. 8, pp. 1-10.
Fonagy, P. & Allison, E. (2014). The role of mentalizing and epistemic trust in the therapeutic relationship. Psychotherapy (Chic).
Fonagy, P. Campbell, C. & Bateman, A. (2017). Mentalizing, Attachment, and Epistemic Trust in Group Therapy. International Journal of Group Psychotherapy, 67: 176–201.
Fonagy, P. & Luyten, P. (2009). A developmental, mentalization-based approach to the understanding and treatment of borderline personality disorder. Development and Psychopathology, 21 (4), 1355-1381.
Fonagy, P. Luyten, P. & Bateman, A. (2015). Mentalizing as Treatment Target in Borderline Personality Disorder. Personality Disorders: Theory, Research, and Treatment Vol. 6, No. 4, 380–392.
Foulkes, S.H. & Anthony, E.J. (1973). Group Psychotherapy: The Psychoanalytic Approach, 2nd Ed. London: Penguin Books.
Hummelen, B., Wilberg, T. & Karterud, S. (2007). “Interviews of female patients with borderline personality disorder who dropped out of group psychotherapy”, International Journal of Group Psychotherapy, Vol. 57 No. 1, pp. 67-91.
Inderhaug, T.S. & Karterud, S. (2015). “A qualitative study of a mentalization-based group for borderline patients”, Group Analysis, Vol. 48 No. 2, pp. 150-163.
Johnson, E.L., Mutti, M.F., Springham, N., and Xenophontes, I. (2016). “Mentalizing after mentalization based treatment”, Mental Health and Social Inclusion, Vol. 20 No. 1, pp. 44-51.
Karterud, S. and Bateman, A.W. (2012). “Group therapy techniques”, in Bateman, A. W. and Fonagy, P. (Eds.), Handbook of Mentalizing in Mental Health Practice, American Psychiatric Publishing, Inc, Washington, DC, London, England, pp. 81-105.
Karterud, S. (2015). Mentalization-Based Group Therapy (MBT-G): A theoretical, Clinical and Research Manual. Oxford, UK, Oxford University Press.
Lewis, L., Kelly, K.A. & Allen, J.G.R. (2004). Restoring Hope and Trust: An Illustrated Guide to Mastering Trauma. Baltimore, MD: Sidran Press.
Linehan, M.M. (2014). DBT® Skills Training Manual, 2nd edition. The Guildford Press, New York.
Lonargáin, D. Ã., Hodge, S., & Line, R. (2017). Service user experiences of mentalisation-based treatment for borderline personality disorder. Mental Health Review Journal, 22(1), 16-27.
Lopez, A., Rothberg, B., Reaser, E., Schwenk, S., & Griffin, R. (2020). Therapeutic groups via video teleconferencing and the impact on group cohesion. mHealth, 6, 13.
Lorentzen, S., Ruud, T., Fjeldstad, A. & Høglend, P.A. (2015). Personality disorder moderates outcome in short- and long-term group analytic psychotherapy: A randomized clinical trial. Br J Clin Psychol. 2 ;54(2):129‐146.
McKenzie, K.R. (1994). Group development. In A. Fuhriman & G. M. Burlingame (Eds.), Handbook of group psychotherapy: An empirical and clinical synthesis (pp. 223-268). New York: Wiley & Sons.
Main, T.F. (1983). The concept of a therapeutic community – variations and vicissitudes. In Pines, M. (ed) The Evolution of Group Analysis. London: Routledge.
Malan, D.H., Balfour, F.H.G., Hood, V.G. & Shooter, A.M.N. (1976). Group Psychotherapy: A long-term follow-up study. Archive of General Psychiatry (33) 1303-1315.
Miller, W. & Rollnick, S. (2002). Motivational Interviewing: Preparing People for Change. New York: The Guilford Press.The National Institute for Health and Care Excellence (NICE). (2009). Clinical guideline [CG78] Borderline personality disorder: recognition and management. NICE: London.
Palahniuk, C. (1997). Fight Club. London Vintage
Pearce, S. and Haigh, R. (2017) The Theory and Practice of Democratic Therapeutic Community Treatment. London: Jessica Kingsley Publishers.
Valentine, S.E., Bankoff, S.M., Poulin, R.M., Reidler, E.B. and Pantalone D.W. (2015). The Use of Dialectical Behavior Therapy Skills Training as Stand‐Alone Treatment: A Systematic Review of the Treatment Outcome Literature. J. Clin. Psychol., 71: 1-20.
Vogt, K.S. & Norman, P. (2018). Is mentalization−based therapy effective in treating the symptoms of borderline personality disorder? A systematic review. Psychol. Psychother. 92 441–464.
Wampold, B.E. (2015). How important are the common factors in psychotherapy? An update. World Psychiatry14:270–277.
Yeomans, F.E., Clarkin, J.F. & Kernberg, O.F. (2015). Transference-Focused Psychotherapy for Borderline Personality Disorder: A Clinical Guide. Arlington, VA: American Psychiatric Publishing.
Gordon Gunnarsen
Group Analyst and Accredited Mentalization Based Treatment (MBT) Practitioner working in the NHS and privately (UK).
gordon.gunnarsen@gmail.com