Birth, Development, and Efficacy of an Outpatient Therapeutic Group for Young Alcohol Abusers
Abstract
The article intends to propose a description of the process and the outcomes of a therapeutic group for young patients of an outpatient service for the treatment of psychological and physical alcohol problems. In particular, the methodological choices are described and illustrated in its aim of enhancing the therapeutic work of the group so that it could become a meaningful context for its members and so that there was a good stability of attendance in the sessions, a good climate and good cohesion. The main contents emerged and the perception of the group climate and the levels of cohesion at different times during 30 group sessions are described. The trial data are then also interpreted with respect to the outcomes that have been measured. Specifically, the difficulty for emotional regulation and the frequency and intensity of craving were assessed in two stages. The comparison between the average values shows an increase in the ability to accept negative emotion, but not yet the ability to manage and control it. There is also an average decrease in the frequency and intensity of alcohol craving. The results are discussed taking into account the process and the different phases of the group which initially involved a tendency of the members to remain in the illusion of a significant change with the emphasis on the value of sobriety, and then give way to expression anger and failure emotions, useful for processing and accepting one’s authentic emotional life underlying the behaviour of alcohol abuse.
Key words: Young alcohol problems, group therapy, nascent state, emotion regulation, group climate, group cohesion
Introduction
Group therapy is one of the most effective methods for treating alcohol and substance use disorders. Much literature has investigated the process factors of a psychotherapeutic group which have the greatest impact on the outcome and effectiveness in relation to the treatment objectives (1, 2). In particular Cohesion and Group Climate are the most frequently process factors (3). According to Yalom (4), these are primary factors for positive treatment outcome. The development of cohesion and group climate in the group context would influence the therapeutic alliance among patients and with the therapist, thus supporting the achievement of the group purposes (5). In addition, numerous studies suggest that, regardless of the theoretical orientation of the therapist, promoting the therapeutic alliance through relational climate and group cohesion has positive effects on treatment motivation and patients’ ability to abstain from psychoactive substances. At the same time, these factors would offer alternative possibilities for regulating emotional states connected with addiction or the underlying affective issues (6, 7).
These findings are particularly pertinent in relation to the involvement of young patients with Alcohol Use Disorders (AUDs) or alcohol dependence in a psychotherapy group conducted in an outpatient service. AUDs and alcohol dependence are frequently associated with greater difficulties in building stable treatment contexts (8). Therefore, the adoption of group management strategies helping the group to become a meaningful context in the minds of the patients, the therapist, the care team and the clinical institution, is of crucial importance.
Building good group cohesion, group climate and alliance also means increasing the level of investment that the members develop towards the group, and consequently allow a regular attendance, oriented to the purposes of the group work. Additionally, a group whose members have a stable and regular frequency increases the sense of security and offers the possibility of positive prosocial experiences and greater involvement in the final goals (9).
To sum up, directly influencing the modulation of the present and future group process guarantees the achievement and maintenance of group cohesion and climate, that in turn lead to greater frequency stability.
This approach begins from considering the group not only as an intervention setting, but also as an entity acting as an agent for change, for which it is fundamental to consider its internal processual evolutionary dynamics (9, 10). We would argue that only when the members attribute meanings to the group, this may become a context where psycho-educational techniques have an effective impact on patients’ choices and on their capacity for self-regulation.
This is the premise for affecting two specific aspects: 1. The evolution from the nascent state, characterized by idealization and dependence on the therapist, to the community of brothers state. This state is based on the recognition of the importance of otherness, allowing for an authentic recognition of one’s own needs and desires (11); 2. The use of techniques and contents which favour the implementation of alternative strategies to the emotional regulation achieved through alcohol.
Study objectives:
This study describes the chosen strategies for the construction and maintenance of good group cohesion and climate, highlighting the effects on the process and several outcomes, including emotional regulation, craving from alcohol use, and frequency of alcohol drinking.
Proposing a Single Case Study, the main objective is to describe the process and the outcome of a psychotherapy group aimed at young patients with AUDs, aged 17-29 years, who turned to the outpatient addiction treatment service. This new therapeutic group for young people was set up in September 2021 as the treatment service provided group intervention only for adults. The proposal of a specific group for young people was based on the evidence that homogeneous groups by age favour treatment motivation, by allowing patients to work towards common goals (12). Specifically, the group aimed to improve three factors: 1. Emotional regulation, 2. Decrease in alcohol craving intensity and frequency, 3. Decrease in drinking frequency.
Group setting description and definition of process-oriented strategies
The choice of the strategies guiding the therapist’s group management starts from considering the dynamics of the development of a nascent group and its evolution as described in literature (11). Literature on group processes identifies four typical phases occurring when a new group sets up 11, 13). Hence, the therapist can define in advance strategic actions and related objectives at each stage, to maximize the possibility that members build and maintain a significant investment in teamwork:
1). The nascent state of the group. This state requires that members get to know each other, that they feel recognized as a group and can develop a sense of belonging. This first phase entails the development of psychic phenomena of mild depersonalization and tendency to use idealization mental defensive mechanism towards the purposes of the group. In this phase, the strategic actions chosen by the therapists and shared with the patients to maximize the development of investment in the group, were:
– The organisation of a kick off meeting, where the potential members met for the first time and were invited to share ideas about their relationship with alcohol and the usefulness of participating in a therapeutic group to stop drinking;
– The organisation of a session in which the patient group met the inter-professional care team (composed by one gastroenterologist, one psychiatrist, one psychologist, one educator, and one social worker);
– The beginning, approximately 20 days after the kick off meeting, of a cycle of 10 weekly group psychotherapy sessions, with the patients who had chosen to participate;
– The organisation of dialogue sessions between the patient group and the inter-professional care team at the end of the 10 session cycle, where patients could renew the interest in participating in the subsequent cycle.
– The choice to close the group and include new members only at the beginning of each new 10 sessions cycle.
The objectives of the strategic actions just described were:
– Strengthening the group boundaries (‘psychic skin’, 14) in the minds of patients and the inter-professional care team;
– Strengthening a sense of group belonging and support the development of group cohesion;
– Promote a first form of group identity, even if characterized by idealization, within an institution that allows it to have a space, a time, and recognition in dialogue with the group of carers.
2). The consolidation phase. This second phase, which began after two 10 sessions cycles (n.20 group meetings), correspond to the “community of brothers state“. In this phase, the group is perceived by its members as a collective subject. The multiplicity of experiences and points of view is increasingly recognized by the participants as a useful resource for a deeper reflection on possible personal changes. In this phase, the strategic actions added to those already listed, primarily regarded the approach in group conductor, the therapist:
– Encouraged spontaneous interactions between members, stepped back and made fewer interventions, in order to regulate group climate or favour the connection of experiences among members (‘bridging technique’, as described in Levine (15));
– Made interventions aimed at facilitating emotional expression and encouraging emotional exchange between members;
– Introduced the use of photographs as mediators to elicit biographic accounts and stories taking the photolanguage method as an example (16).
The objective of the above actions was to support and consolidate the group as a whole, which is more than the sum of the individual parts (17) and which, as a collective subject, is closely connected to its own objectives of change and recovery.
3). The intermediate phase. After having built a solid ‘container’, clear boundaries, mutual trust, and the recognition of one’s own emotional life outside the mechanisms of depersonalization and idealization, the group is ready to welcome the events occurring in members’ daily lives. The group is able to analyse such events in an objective way, and to use them to share doubts and difficulties. In this phase, therefore, the strategic actions envisaged by the therapist were:
– Conduction oriented to explore interpersonal events and happenings of the here and now in the group, and of the daily life of the patients;
– Offering a space to discuss possible relapse into alcohol use or experiences of failure;
– Encouraging members to bring a narrative regarding what was happening in their lives;
– Promoting expression of difficult emotions, such as anger and disappointment.
The objective was to prepare the way for the introduction of alternatives in emotional regulation related to everyday events.
4). The intensive phase. In this phase, the group members are ready to accept the proposal of psycho-educational methodologies and strategies, as they have built in their mind a “meaning frame” of what happens in the group and how much group belonging can support their ability to decide how to manage their emotional life.
The strategic actions of this phase were therefore oriented to propose mentalization and emotional regulation techniques of different types. These included:
- “Moviola” technique (18) to analyse and mentalize mental states related to a specific interpersonal event;
- Self-regulation techniques;
- Techniques for monitoring one’s addictive behaviour
The objectives of these techniques included the promotion of personal capacity for emotional self-regulation, by proposing the group as a ground for experimentation and learning. In this phase, the inclusion of new members allowed the older members to consolidate their sense of self-efficacy. In addition, the existing group culture promotes the transition of new members to further motivational stages.
Group composition
The group was initially composed of six members, four males and two females. Of those who participated in the inaugural event, only one did not start the first cycle (October-December 2021), while the others gave their confirmation. The second cycle (February-May 2022) saw the insertion of 4 other members, while the third cycle involved eight members in total. The ages ranged from 17 to 28 years, and the primary diagnosis for all was “Alcohol Use Disorder”, for three of them in conjunction with Cluster B and Cluster C Personality Disorder. The group concluded the intermediate phase in July 2022 and it is expected to enter the intensive phase in October 2022. The therapeutic team will propose to work in a more targeted way on emotional regulation techniques.
Tools and Method
A range of qualitative and quantitative tools were chosen to verify the set objectives:
For the evaluation of the process the following were used:
- Clinical observation of the process, starting from the writing of detailed reports on the contents of each session, conducted by a trained observer;
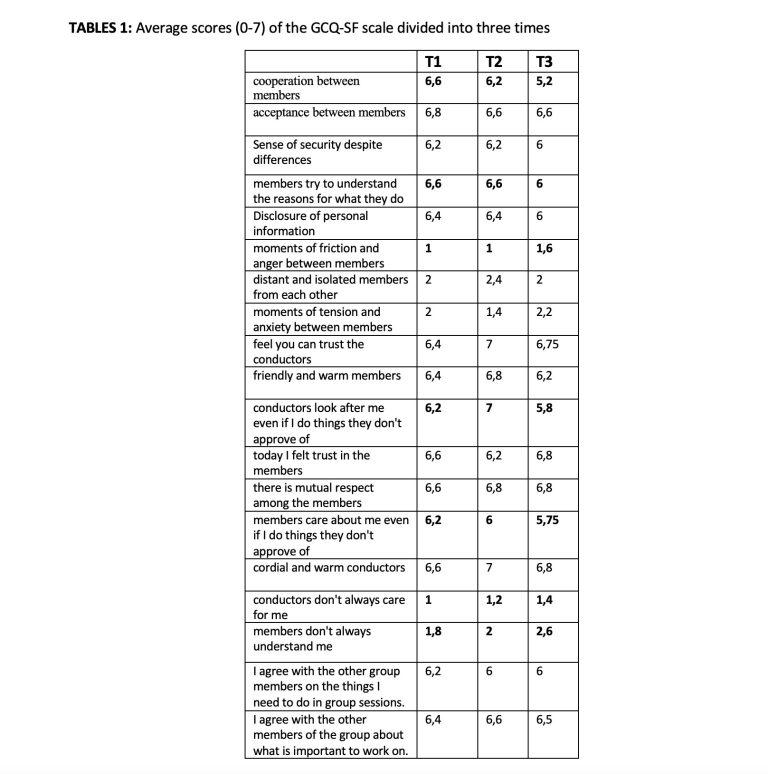
- Questionnaire on group climate (GCQ-SF, (19)), consisting in 12 statements concerning the relationships among members and the relationships with the group leaders (degree of agreement on a scale ranging from 0 to 6). The questionnaire was administered at three different times (nascent, consolidation and intermediate phase);
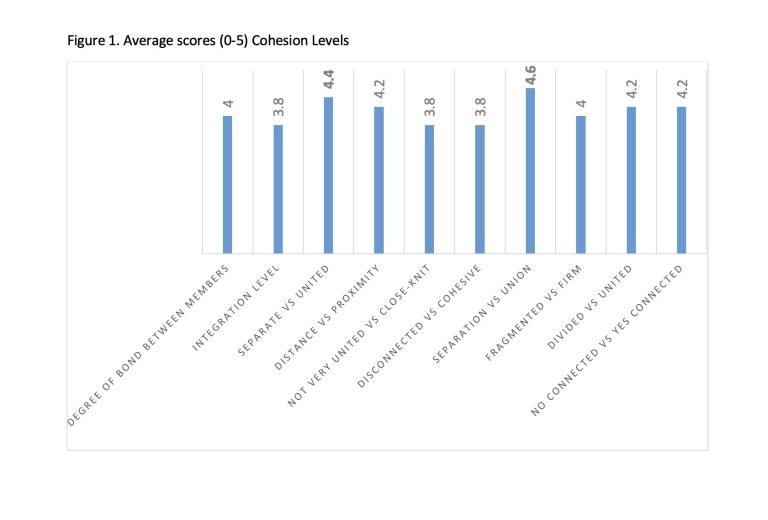
- Unitary Cohesion Index (IUC, (3)), which presents a list of 10 adjectives (eg., the group is linked/united; united/separated; attached/detached etc.) in a double semantic pole scale, for each of which respondents are asked to indicate their position (from 1 to 5) with respect to the perception they have towards the group. The group cohesion scale was administered at the end of the intermediate phase;
- Process indicators such as the average number of sessions attended and the number of dropouts (voluntary non-agreed interruption of attendance at the group and at the service).
The outcome evaluation was detected with self-report tools:
- DERS Scale (Difficulty Emotion Regulation Scale, Italian adaptation (20)) administered at the beginning of the consolidation phase and at the end of the intermediate phase. DERS is a 36-item scale, with response modalities on a 5-point Likert scale (from 1 = almost never to 5 = almost always), which evaluates the amount of difficulties in regulating emotions according to six constructs: 1.Acceptance difficulty, that is the tendency to experience negative secondary emotions in response to one’s negative emotions; 2. The difficulty in distracting oneself from emotion and performing alternative behaviours, that is, this difficulty predicts the inability to perform a goal-oriented behaviour for adaptive purposes; 3. Lack of confidence in one’s own emotional regulation skills; 4. The difficulty in maintaining control over one’s behaviour when experiencing negative emotions; 5. The difficulty in recognizing the emotion one is feeling; 6. The degree of attention paid to one’s emotional state. Subsequent administrations will be scheduled every 5 months, and administered to each new member at the entry into the group;
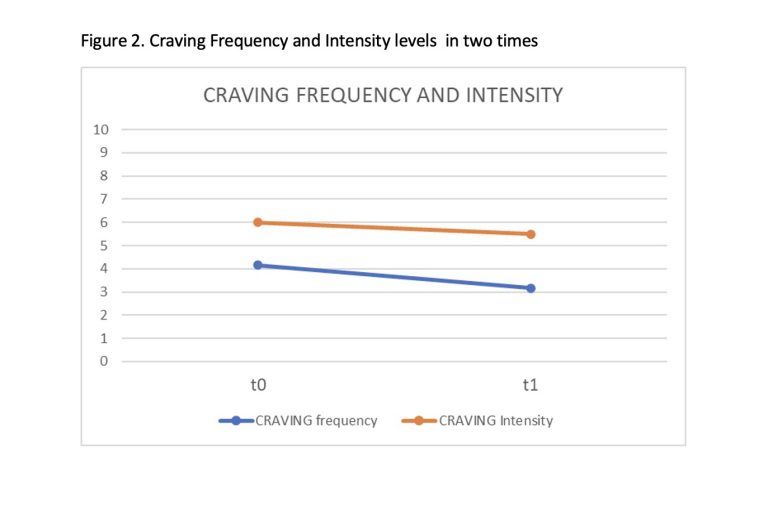
- The alcohol craving frequency and intensity scale, which investigates on a scale from 0 to 10 how many times in the last 10 days the respondent felt the urge to drink and how intense this desire was. This tool was administered together, twice, with the previous one.
- The accounts elicited by a set of photographs, used as mediators, to answer the question: “How do others see me? Tell me with a photo”. This technique, employed at the Consolidation and Intermediate phase, intended to explore the changes in participants’ mentalization over time and in describing themselves through their hypotheses of how others would describe them. These findings will not be considered in this work.
Analyses
Process Analyses: A thematic content analysis was conducted on the transcripts of the sessions. The therapist and the observer identified prevailing themes for each phase of the group, using a prevalently inductive process. Themes were progressively refined and validated through discussions within the research team, where the intersubjectivity of meanings was tested. made by identifying the prevailing themes for each phase of the group, through a comparison between the conductor and the observer, and in addition to external observers who knew the group only through the transcripts.
Outcome Analyses: The analyses of the self-report tools were carried out with calculation of the averages and qualitative comparison of the average values between the different administration times. No parametric statistics were performed due to the limited number of subjects.
Results
This section presents the aggregated results collected from the group participants. Here, we will not focus on individual-level changes, as this would require a clinical study approach which is beyond the objectives of this study. The results are summarized in two parts: process analysis and outcome analysis, both resulting from the cross-reading of qualitative and quantitative data.
The process analysis considers the following aspects: 1. Thematic content of transcripts and notes 2. Measurements of group climate, 3. Measurement of cohesion levels.
1). The thematic contents of the nascent state highlight an idealization of the group and, simultaneously, its change. Participants’ accounts frequently regarded their capacity to totally abstain from alcohol, unlike friends in their life context, who continued to drink, sometimes at harmful levels. Sobriety was often evoked in speeches as a myth to be achieved, a value, or an idealized aspect. Participants also resorted to the binary distinction “inside/outside” the group. In this way, they seemed to consolidate their sense of belonging and define the group boundaries. In the consolidation phase, however, biographic stories were more frequent. These aimed at deepening a mutual and authentic knowledge, which favoured the emergence of further stories. Finally, the intermediate phase saw more frequently the recurring of narratives regarding present or past episodes of relapse, and the experiences of disappointment and failure, with consequent actions.
2). The measures of the group climate shows a constant trend from the baseline to the three follow-up points (Table 1) in maintaining high positive levels of the group climate (beyond level 5), and in keeping the negativity levels low, in almost all the different aspects reported by the items. In the nascent state, the values related to the spirit of acceptance among the members and those related to cooperation, understanding, trust and respect are the highest. In relation to the conductors, cordiality is the most appreciated quality.
Then there are aspects such as the sharing of work objectives, personal information and trust towards the conductors. On the other hand, the detection of anger and distance and neglect on the part of the conductors are at minimum levels. In the subsequent two phases, consolidation and intermediate phases, cooperation between the members tends to decrease to leave space to the detection of anger and the perception of not being sufficiently understood by the members. However, levels for anger are low, levels for the sense of acceptance among members sufficient. These shifts in the values in some items reveal how the group climate consolidated through the trust in the leaders and, at the same time, a greater expression of anger and difficulty in cooperation and understanding between the members without, however, a lack of respect and acceptance. This may also indicate greater authenticity in the relationships between members after the end of the illusory phase of the nascent state. In addition, there seems to be a shift towards a common sharing of group work goals, with a parallel feeling of receiving lower approval from the therapist and members in case of actions challenging shared change goals. Trust and respect towards the conductors and towards the members remain the aspects that maintain the highest levels in the last phase considered.
3). Group Cohesion was detected at the end of the last phase (intensive phase). The graph shows the averages of the continuum that separates a pole of meaning from its opposite. Above all, the perception of a dichotomy: union vs separation emerges. The group members seem to perceive that the group tends to remain connected despite the occasional lack of harmony and integrity. In this case, therefore, cohesion is determined by the fact that the group can be a secure basis, the starting point for the elaboration of the separation/identification phase. The sum of the answers of all adjectives can range from a minimum of 10 (low cohesion) to a maximum of 50 (high cohesion). In this case study, the average score obtained is 41 (the average of the sample with which it was validated the scale is 36.41, SD= 8.06).
4). Finally, the average number of sessions performed by each participant for each phase was 27/30, which represents very high adherence levels. Previous results about cohesion rates are confirmed by the stable attendance of each member. Two participants dropped out, and two participants did not complete the treatment due to relocation and new work commitments.
The outcome analysis. Graph 2 reports the average scores related to each of the subscales that indicate the degree of difficulty of emotional regulation (the higher the score, the higher the difficulty) at the two survey times, the first in the intermediate phase and the second in the intensive phase.
Interestingly, the highest improvement seems to be related to the difficulty of acceptance, or in the intensive phase it seems that there is a lower tendency to develop a negative emotional reaction following the conscious emergence of a negative emotion. Therefore, the acceptance of the suffering characterising the emotional life of young members who abuse alcohol seems to be the aspect with the greatest impact on group process described above. However, the acceptance of one’s negative emotional life does not correspond to the ability of managing it, favouring at first impulse discontrol, and the tendency to ward off from it. A greater ability to recognize emotions may more easily lead to the use of avoidance strategies. The ability to accept negative emotion, however, seems to be an important motivational precursor at the beginning of a phase, when participants may be more ready to learn and implement effective techniques of emotional regulation. Finally, a decrease in average levels of alcohol craving and frequency and intensity of craving episodes can be observed (See Figure 2)
Discussion
The results presented allow to make an integrated clinical reading between the process and the outcomes, enriching the elaboration of work hypothesis and a deeper understanding of what happens in a group.
The content analysis and the result of the questionnaire on group climate suggest that the initial strategies aimed at building the group boundaries may have favoured a significant investment in the group. The frequent themes of idealization towards sobriety as a founding value of the group members, and the high levels of acceptance, cooperation and mutual trust, seem to have prepared the ground for subsequent events which, especially starting from the intermediate phase, allowed for a greater expression of negative emotions such as anger. The quality of the relationship among members decreases in the perception of cooperation, but this does not call into question the cohesion and belonging to the group. This latter seems to be increasingly structured towards a greater sharing of work objectives. The group “container”, which has gradually been defined in the minds of patients and the team, has increasingly acquired a meaning oriented towards therapeutic work and the development of the evolutionary processes of individuals.
The work conducted during the nascent state and the strategies oriented to the construction of a group identity within an institution which recognise it as the group of young people in dialogue with the multi-disciplinary care team, allows patients to build a partial identity, linked to group belonging , and offers them affective, emotional and behavioural reference points, useful for restarting an evolutionary process. The restarting of a growth mechanism passes through mirroring in the other members and helps self-acceptance allowing members to find the words to describe their emotional life that is gradually placed and re-signified by interpersonal events that occur in your daily life.
It is important that the group context is constituted in the minds of patients as a safe place where they can express their differences and their way of suffering and communicating. This result, however, is more difficult if a careful and structured management of the groups processes is poor or lacking.
Conclusion
This study proposes a reflection on the dynamics and strategies to build a therapy group which could represent a fertile and meaningful ground for young people with Alcohol Use Disorders. However, the interpretation of research results at the moment can only provide hypotheses, which need to be tested through further empirical research. This might provide further evidence regarding the effectiveness of the group settings for the cure and treatment of psychic and behavioural problems related to alcohol abuse and dependence.
References
1). Vasta FN, Girelli R, Gullo S, (2013) What homogeneity in the groups? Elements of theory, clinic and research. (first edition) Alpes Eds.
2). Wagner CC, Ingersoll KS, (2013) Motivational Interviewing in Groups. Guildford Eds
3). Donelson RF, (2021) Recent Advances in the study of Group Cohesion. Group Dynamics, Theory, Research and Practice. 25:213-228.
4). Yalom ID, (1995) The theory and practice of group Psychotherapy. New York Basic Books 4th
5). Alldredge CT, Burlingame GM, Yang C, Rosendahl J, (2021) Alliance in group therapy: A meta-analysis. Group Dynamics: Theory, Research, and Practice 25(1): 13-28.
6). Stinchfield R, Owen PL, Winters KC, (1994) Group therapy for substance abuse: A review of the empirical research In Fuhriman A, Burlingame GM, Handbook of Group Psychotherapy: An Empirical and Clinical Synthesis. Wiley eds.
7). Flores PJ, (2004). Group psychotherapy with addicted population: An integration of Twelve-Step and Psychodynamic Theory. Haworth Addiction Treatment. New York: The Haworth Press.
8). Yalom I, Leszcz M, (2020) The theory and practice of group psychotherapy Basic Books 5 th Eds
9). Weinberg H, Rolnick A, (2022). Theory and Practice of Online Therapy. Internet-delivered interventions for individuals, Groups, Families, and Organizations. Routledge Eds.
10). Weinberg H, (2022). Interview with Molyn Leszcz. In: Theory and Practice of Online Therapy. Internet-delivered interventions for individuals, Groups, Families, and Organizations. Routledge Eds
11). Neri C, (2017). Group (second edition). Raffaello Cortina Eds.
12). Ewing SW, Walters ST, Baer JS, (2013). In Wagner CC, Ingersoll KS, Motivational Interviewing in Groups. Guildford Ed.
13). Neri C, (2021). The group as a cure. Raffaello Cortina Eds.
14). Anzieu D, (1989) The Skin Ego Karnac eds
15). Levine R, (2017) A Modern Psychoanalytic Perspective on Group Therapy, Int Jou Group Psych, 67: sup1
16). Vacheret C, (2004) Photolangage: a group method with a therapeutic or formative view. Funzione Gamma, 426. funzionegamma.it
17). Lewin K., (1948). Resolving Social Conflicts: Selected Papers on Group Dynamics. New York (Trad. It. I conflitti sociali. Franco Angeli: Milano 1972).
18). Esposito G, Formentin S, Marogna C, Sava V, Passeggia R, Karterud SV (2022), Pseudomentalization as a Challenge for Therapists of Group Psychotherapy With Drug Addicted Patients, Front Psychol 4;12:684723
19). Costantini, A., Picardi, A., Podrasky, A., Lunetta, S., Ferraresi, G., & Balbi, A. (2002). Group Climate Questionnaire: validation of a process measure for group psychotherapies. Journal of Psychiatry, vol. 37, n.1.
10). Sighinolfi C, Norcini AP, Chiri LR, Marchetti I, Sica C, (2010). Difficulties in emotion regulation scale (DERS): the Italian translation and adaptation. Psicoterapia Cognitiva Comportamentale 16(2):141-170.
Author Affiliations
Silvia Formentin: PhD, Individual and Group Psychotherapist, Addiction Department, Aulss 6 Euganea, Serd UOC Padova and Piove di Sacco, Padua, Italy
Alessia Grigolin: Professional socio-health educator, Dependence Department, Aulss 6 Euganea, Serd UOC Padova and Piove di Sacco, Padua, Italy
Salvatore Lobello: Medical Gastroenterologist, Food Science Specialist, Director of the Simple Operating Unit of Alcology Problems, Addiction Department Aulss 6 Euganea, Serd Padova and Piove di Sacco, Padua, Italy
Cristina Marogna: Psychoanalyst SPI- IPA. Associate Professor, Department of Philosophy, Sociology, Education and Applied Psychology, University of Padua, Padua, Italy
Mascia Ortolan: Psychiatry Specialist, Addiction Department AUlss 6 Euganea, Serd UOC Padova and Piove di Sacco, Padua, Italy
Serena Vicario: PhD, Social Worker, Addiction Department, AUlss 6 Euganea, Serd UOC Padova and Piove di Sacco, Padua, Italy
Giancarlo Zecchinato: Specialist in Psychiatry, Director of the Addiction Department UOC, Aulss 6 Euganea, Padua, Italy
Corresponding Author

Silvia Formentin, Addiction Department Ulss 6 Euganea, via dei Colli, 4 35100 Padova. Tel. 049 8216016; Cell 349 5696337; silvia.formentin@aulss6.veneto.it